Mechanical ventilation for people with motor neurone disease (MND) is a sensitive and little discussed topic. Yesterday’s respiratory management session of the International Symposium on ALS/ MND began with several interesting and thought provoking presentations on the subject. Pia Dryer from Aarhus University Hospital in Denmark presented the results of a review of their respiratory service over 17 years, including a discussion of invasive ventilation. Dr Mike Davies is a respiratory consultant at the Papworth Hospital in Cambridge in the UK, where he and his colleagues run a weaning service supporting people to come off invasive ventilation.
Choosing ventilation, or not
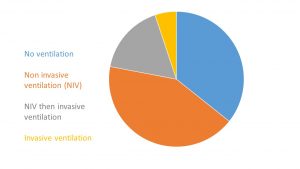
Over 400 people with MND had been treated at the Home Mechanical Ventilation service since its inception in 1998, Pia Dryer explained at the beginning of her talk. During the discussions in clinic people had the choice about the options available for managing their breathing symptoms, some chose no ventilation, others non-invasive ventilation (NIV). From NIV some then progressed to invasive ventilation or tracheostomy, and finally some chose to go straight to invasive ventilation. People with MND had the choice of all of these options, 90 of them chose either NIV and then invasive ventilation or invasive ventilation first without NIV. The talk was really brought to life by showing clips of Birger Bergman Jeppesens the star of a number of films on YouTube. He was the first patient to ask for invasive ventilation at the Aarhus clinic. Dr Dreyer went on to talk about the legal and ethical aspects of withdrawing ventilation from people with MND at the end of life, a topic that was discussed in more depth later in the session.
Sudden and unexpected development of breathing problems

The next speaker, Dr Mike Davies, highlighted a very different issue about people who were invasively ventilated in an emergency. He began by reviewing the experience of the service in the last 12 years, including some information on how and why people came to be invasively ventilated in the first place.
He explained that difficulties in breathing in people with MND can come on very suddenly, starkly illustrated by the fact that a healthy, exercising person will move 100 litres of air per minute through their lungs, whereas someone in a wheelchair will be moving as little as 5 litres per minute. He commented that below 5 litres a minute, serious respiratory problems occur. The effects can come on suddenly meaning that some people may be given an unplanned tracheostomy in intensive care. In a few rare cases, people may not have a diagnosis of MND at this point. After the ventilator has been inserted, it may be many months before they leave the intensive care unit, while the care and support they need is arranged.
Unplanned invasive ventilation is not a one way street
From this very bleak picture, Dr Davies gave some hope. He explained that the Papworth weaning service were able to successfully wean many people with MND from invasive ventilation to non invasive ventilation, allowing people to return home. The proportion of people that Papworth are able to discharge home compares very favourably to reviews of other weaning services across the world. It is a success he attributes to the team around him, commenting “It is the people who deliver the service, that’s where the magic is at“.
You can find more information on the management of respiratory and breathing symptoms on the MND Association website.





Little discussed topic matters in some occasions. Nice analysis.