
Research into genetic causes of MND has greatly increased over the last few decades and gene changes have since been found to play a role in both inherited and non-inherited (sporadic) forms of the disease. Since the discovery of the first gene change in MND around 30 years ago, researchers have found over 40 gene mutations that play a role in the development and progression of MND. It is highly likely that there are more gene changes that could be involved in the disease which are still being researched or are yet to be discovered. Understanding more about gene changes in MND will allow us to gain more insight into what goes wrong in the neurons in MND and find ways that these faulty genes may be corrected.
We recently organised the 34th International Symposium on ALS/MND held in December in Basel, Switzerland. The symposium allows researchers, healthcare professionals and people with MND from across the globe to come together to discuss the very latest updates in MND research. Similar to previous years, genetics played a large role at this year’s symposium with 5 talks given and over 30 posters presented. Topics discussed ranged from how different gene changes are more frequent in different populations of people to how some gene mutations may impact someone’s disease progression and survival.
Genetics and MND really came into the spotlight in the closing session of the 34th International Symposium and we wanted to share some of the work presented in this session with you.
Improving Genetic Testing results
As we discover more gene changes which may play a role in MND, it is important that we are able to test for these changes and accurately determine whether someone has a gene mutation that may be the cause of their MND. Genetic testing is becoming more crucial as more therapies designed to target gene mutations in MND are being developed and tested in clinical trials. Testing for gene changes that are known to be involved in MND could help identify whether people are able to take part in these trials and, if the therapies are approved, make sure people can access them quickly.

During the closing session, Dr Matthew Harms from Columbia University Irving Medical Center discussed the importance of genetic testing in MND and highlighted some of the current barriers to this testing. At the moment, there is little research into why these barriers might exist and how they can be overcome.
One of the current barriers to genetic testing is that some clinicians feel that they need more support with knowing how to interpret the results. Genetic testing might show that someone has a gene change linked to MND but it can be hard to know if it may be a cause, increase someone’s risk of developing MND or influence disease progression.
Dr Harms co-founded the Clingen ALS gene curation expert panel which is an international panel of 19 experts from 8 different countries across 5 continents. This panel is made up of a mix of genetic counsellors, clinicians and researchers working in the field. The aim of this panel is to improve the interpretation of genetic testing results by determining how significant MND gene changes are in the development of the disease. This involves the panel reviewing all of the available data for each gene change and classifying the change based on how likely it is to be a cause of MND. They look at several different aspects of the data and give scores which determines how likely the gene change is to play a role in MND. The individual scores by each panel member are then discussed by the whole panel and they make a final decision on the classification of the gene based on it’s likely involvement in the disease.
Over 29 months, the Clingen ALS gene curation expert panel reviewed gene data and were able to reclassify 42 out of the 45 genes that have been found to be linked to MND.
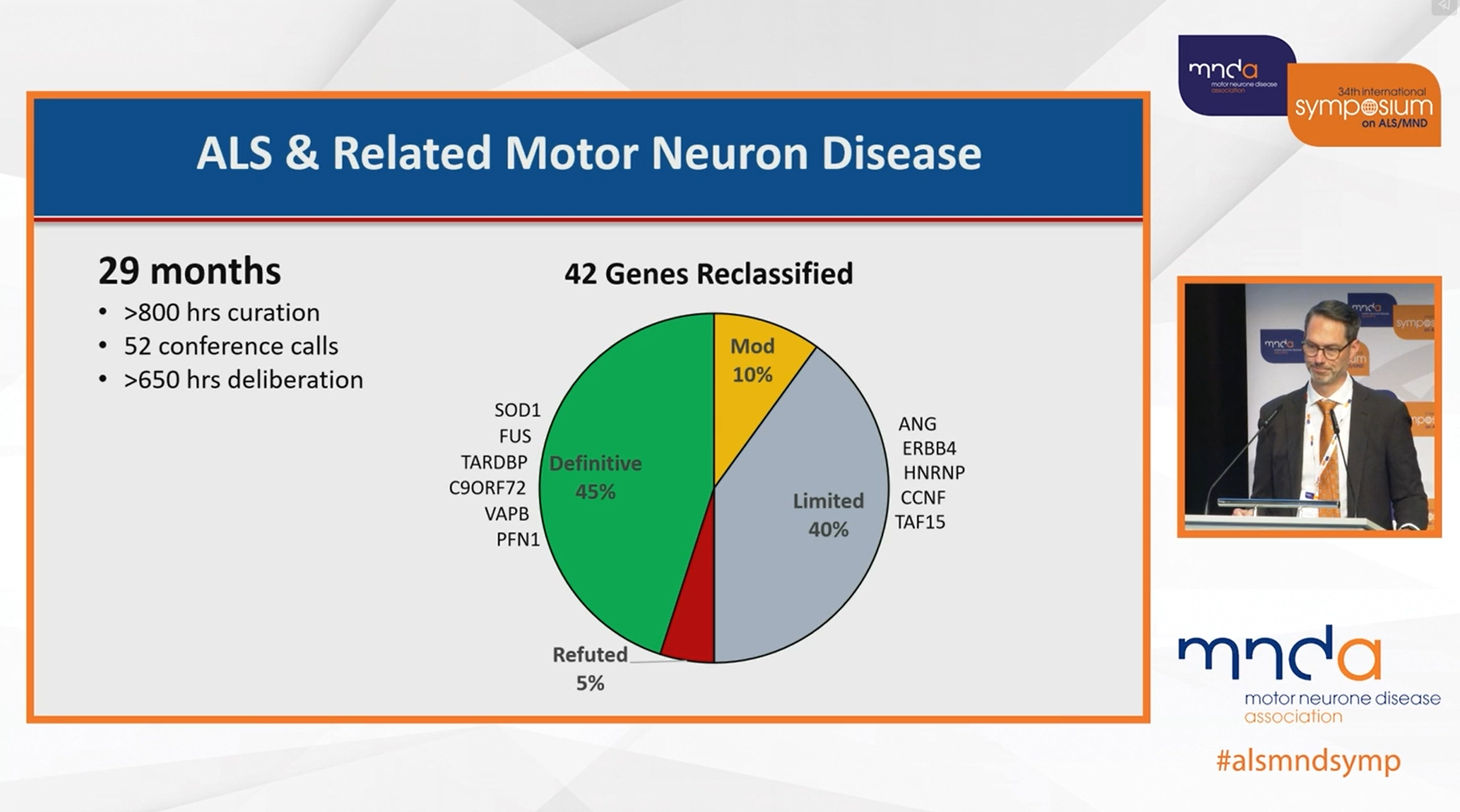
Being able to confidently reclassify these genes means that the results of genetic testing can be more accurately reported. There can be recommendations made that genes in the limited or refuted classifications (where current evidence suggests they are unlikely to be causes of MND) are not included in genetic testing or are not reported in results. If these genes are still tested for, then the results could highlight that there was a mutation found in this gene but there is limited evidence that it is a cause of MND at this point in time.
This work is also important in helping clinicians to better understand genetic testing results and feel more confident in interpreting them. It helps to provide more accurate information for people who have had genetic testing and allows clinicians to make sure people who are eligible for approved gene therapies are given the option to have them.
Classifying genes in MND could also be helpful in prioritising which research to fund in the future as funding could be directed towards projects looking at those genes in the limited classification to gain more evidence and data to review. This may enable a final decision to be made on whether they play a role in causing MND. We look forward to hearing more about the work of the Clingen ALS gene curation expert panel and the reclassification of genes involved in MND.
A new type of potential gene therapy
Genetics also featured in the late-breaking news section of the closing session. Professor Pietro Fratta shared the work of his group at University College London on the development of a new potential gene therapy for MND and frontotemporal dementia (FTD). This new technique uses biology that is known to go wrong in neurons in MND/FTD and exploits it to increase the levels of proteins that are usually decreased in diseased motor neurons.
TDP-43 is a protein which has been found to be faulty in 97% of cases of MND and FTD. It moves outside of the cell control centre (the nucleus) to the cell body (cytoplasm), causing its ability to regulate the instructions which make proteins to be lost. This means that the instructions can contain pieces of information that are not needed to produce the protein, called cryptic exons. This new potential gene therapy relies on these cryptic exons being included, and uses the cryptic exon against itself, to kickstart the cell to make a specific protein which is usually reduced in the disease.
Gene therapies can cause ‘off target effects’ as they work in every cell in the body, even healthy ones, and don’t just target those damaged by the disease. In MND, it may be that only a handful of neurons are diseased and most are still healthy. Gene therapies allow the diseased neurons to be treated but may cause toxic effects to the healthy neurons in the long term.
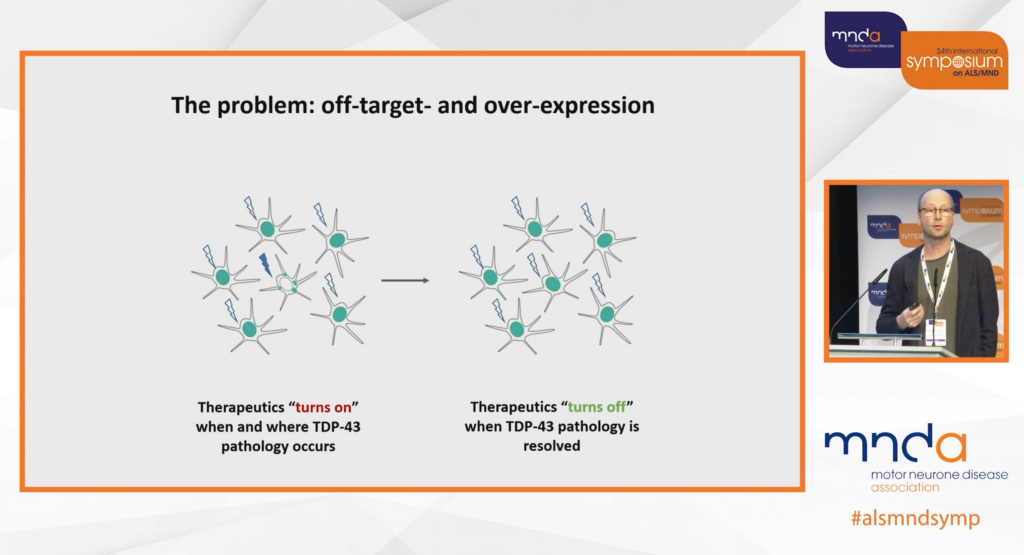
Professor Fratta’s lab have designed this possible new gene therapy to be delivered to all cells but to be ‘switched on’ when the damage begins in the cell and ‘switched off’ when the cell has been treated and the damage is gone. This approach means that the possible gene therapy only acts in cells that are affected by the disease and only when TDP-43 becomes faulty. This means that it could potentially be given to people who are at higher risk of developing MND/FTD before symptoms appear but would only work once damage starts and may prevent damage from spreading. The potential gene therapy could help to reduce the toxic effects of faulty TDP-43 in neurons and restore protein levels in MND/FTD. This therapy is currently still being tested in the laboratory and we are excited to see how this work develops.
And the award goes to…
During the closing session of the symposium, there were two awards that were given to researchers working in MND who have made significant contributions the field. Both of these awards went to teams of researchers who have helped to drive forward new gene therapies for MND.
The Sean.M Healey International Prize for Innovation in ALS is awarded to a team of researchers who are working on new technologies which help to develop new treatments for the disease. This year, the prize was awarded to the international team of researchers who have helped establish neurofilament as a biomarker of MND.

This international team have worked together to build guidelines for collecting samples from people with MND, develop ways to share data from these samples across countries and create a method that allows neurofilament to be measured accurately in any laboratory. They have been able to show that neurofilament levels rise in MND and are different depending on the person’s disease progression. Those with faster progression have higher levels of neurofilament than those with slower disease progression. The team have also shown that levels of neurofilament start to rise before symptoms of MND appear and this may be useful in monitoring people who are at risk of developing MND to see when the disease starts in neurons.
Neurofilament has now been incorporated into many clinical trials to help measure whether new potential treatments are able to reduce levels of the protein, which could mean it is slowing the progression MND. This was used in a clinical trial of a gene therapy for SOD1 MND called Tofersen. The trial results showed that those who were given Tofersen had decreased levels of neurofilament compared to those who were given a dummy drug. This data was critical in the approval of Tofersen as a treatment of SOD1 MND in the USA. Tofersen is currently only approved for use in the USA and is only beneficial for people with MND who have a mutation in the SOD1 gene.

RELATED POST
Blog | 26 April 2023 | Charlotte Roy
What does the FDA approval of Tofersen mean for the UK MND community?
The Lalji Family award is awarded to a team of researchers who are looking at ways to improve the repair of damage to neurons in MND and help people with the disease to regain some of the function which has been lost. This year, the Lalji Family award was won by the team of international researchers behind Jacifusen (ION363), a potential gene therapy for people with mutations in the FUS gene.

FUS MND usually affects children and younger adults and the disease typically progresses very quickly. This team of researchers worked together to create models of FUS MND so that the effects of the gene mutation could be studied in the laboratory and increase understanding of the biology of this form of MND. Through studying the changes in the FUS gene in the lab, the team helped to identify that FUS becomes faulty in MND and behaves in a toxic way in diseased neurons. They also found that having no FUS in cells does not lead to motor neuron damage. This led to the development of a gene therapy which aims to silence the FUS gene in people who have FUS MND as this stops the toxic action of FUS in the disease. This potential gene therapy, called Jacifusen, is currently being tested in a clinical trial and there are 18 people who are now receiving the therapy as part of an expanded access program (which gives people who are not able to take part in the trial access to the potential treatment).
RELATED POST
Blog | 26 April 2023 | Charlotte Roy
Silence is golden: A new clinical trial for FUS-ALS
One of the people receiving Jacifusen on the program, Anna, came on stage with her mum to tell her story and talk about how treatment with Jacifusen has helped her regain some function. Anna was diagnosed with FUS MND at aged 16 in 2020 and began treatment with Jacifusen two months later. Anna continued to lose function for the first few months on the treatment (which can be seen by her ALSFRS score on the graph below) and in August 2021 she was hospitalised and was locked in her own body. She continued the treatment and began to improve and can now stand and walk again.
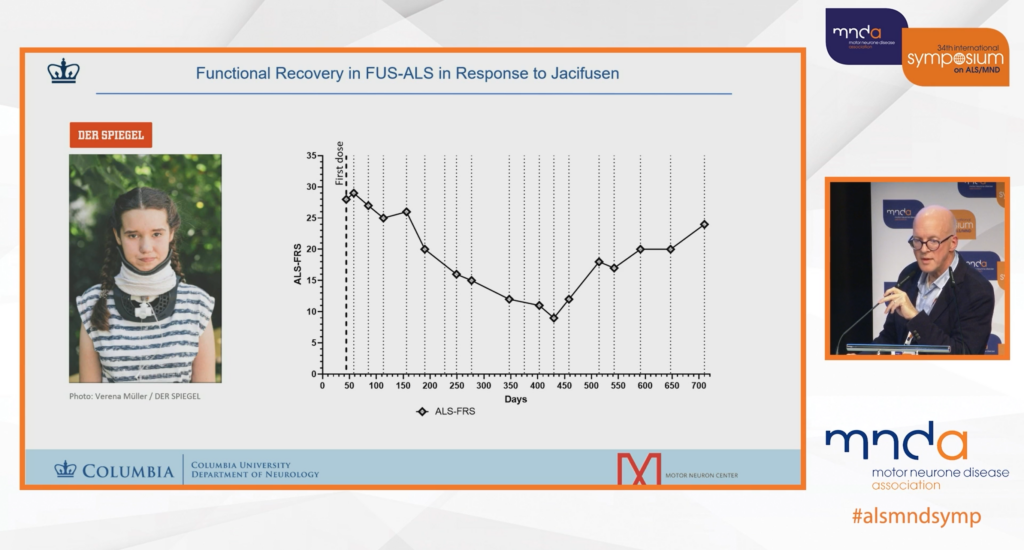
She has now been living with this very aggressive and rapidly progressing form of MND for over 3 years due to treatment with Jacifusen. Anna’s story filled the room with emotion and inspiration. The entire audience was on their feet to applaud her and the success of the team behind her treatment. Her closing slide lit a fire in everyone in the room as she voiced a common goal among the community that “There will be a cure one day!”.
The scientist in me says we have to complete the trial to prove that this drug works. The clinician in me says the proof is behind me (Anna).
Dr Neil Shneider, Columbia University
Research into the role that genetics play in MND has hugely increased over the last few decades and there are now several global databases collecting genetic information about MND. Identifying new gene changes, and confirming known gene changes, that could contribute to the cause of the disease will lead to more gene therapies being developed. There are now several clinical trials of gene therapies happening around the world and the first ever gene therapy for MND, Tofersen, was approved for use in the USA last year. It is hoped that more effective gene therapies will emerge in the years to come and give better treatment options for people with MND, and possibly be able to delay or prevent symptoms in those at higher risk of developing the disease due to gene mutations.