
A paper arising from research carried out at the University of Sheffield as part of the AMBRoSIA biobank, and in collaboration with the international Project MinE gene-hunting consortium, was recently published in the Journal of Neurology, Neurosurgery and Psychiatry. Researchers propose that a test for the most common MND genes could be offered to all patients in the future, whether they have a family history of the disease or not. This could have a positive impact on care and provide more opportunity for involvement in ‘personalised’ clinical trials, with the development of new therapies targeting specific genetic forms of the disease.

AMBRoSIA (A Multicentre Biomarker Resource Strategy in ALS), a five-year biobanking programme funded by the MND Association, began with recruitment of the first participant in June 2017, and aim is gathering biological and genetic samples from several hundred people with MND, as well as donors without the disease in the UK. It is the largest project that we have ever funded (see our previous AMBRoSIA blog) and we believe this valuable resource of UK MND samples will form the basis of many significant research studies, including developing our understand the various types of MND and the identification of biomarkers that could be a signature of the disease.
Recruitment for the study took place at three sites throughout the UK – Sheffield (headed by Prof Dame Pam Shaw), Oxford (headed by Prof Martin Turner) and London (headed by Dr Andrea Malaspina). In addition to AMBRoSIA, its sister project – NECTAR, also funded by the MND Association, is conducting comprehensive genetic screening for the participants taking part in the AMBRoSIA study – led by Dr Janine Kirby at the University of Sheffield and Dr Pietro Fratta at University College London. It is humbling to see the generosity and commitment of people with and affected by MND selflessly gifting samples to the study, helping in the fight against the disease.
What did the study show?
In this study, the first 100 MND patients enrolled to AMBRoSIA had the genetic sequence of 44 MND-relevant genes (previously known to be associated with MND) ‘read’ from their genomes (DNA). The genes were analysed in detail to look for any changes/errors in the sequence of each gene compared to the same gene in people who do not have MND.
Interestingly, the researchers found higher than expected genetic changes in the group of patients.
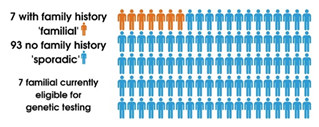
Initially seven of the 100 participants had a family history of MND (orange people in graphic) and 93 did not. This corresponds to what is thought currently that 5-10% of MND cases are referred to as ‘familial’ if there is a clear family history of MND and/or frontotemporal dementia (FTD), while the majority of MND cases are considered sporadic (with no family history and no identifiable cause).
In the UK currently, only patients with a family history of MND, dementia, or who experience disease onset at a young age are routinely offered genetic screening in the UK. This means that only seven percent of people would usually be offered genetic testing to see if they carried a faulty gene and the remaining 93 would not.
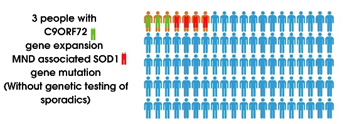
Firstly if we look at the familial cases only, the 7 cases had variants in either the SOD1 (red clothes in the graphic) or C9ORF72 (green clothes in the graphic) genes.
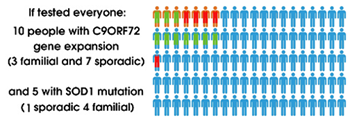
However, looking across all 100 participants, 15 actually had a change in either SOD1 or C9ORF72 genes.
As expected, the most frequently identified likely disease-causing mutation was in the C9ORF72 gene, found in 10 of the 100 people (3 familial cases and 7 sporadic). Five SOD1 cases were seen, of which 4 were familial and 1 was sporadic. In principle, this suggests that if all participants were genetically tested, a further 8 people who were classed as ‘sporadic’ would potentially meet the criteria to take part in one of the current MND genetic-therapy trials as they also had particular genetic changes in either SOD1 or C9ORF72.
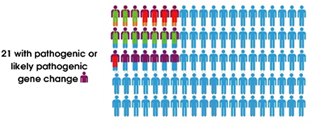
The researchers found that 21 of all participants had mutations in the known risk genes (purple t-shirts) which was either known to be or likely to be associated with the disease (pathogenic). Of which, 14 had no family history of the disease (sporadic). Of these 14 sporadic cases (without orange trousers in the graphic), one had a SOD1 mutation and seven had changes in the C9ORF72 gene.

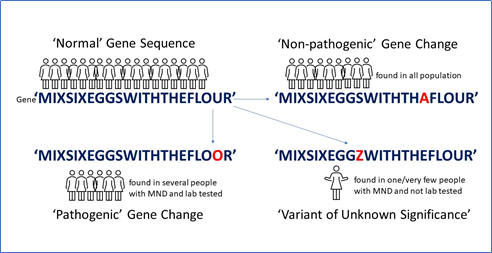
An additional 21 sporadic participants (pink t-shirts) had changes in genes associated with MND but at a place in the gene sequence that we don’t know whether it is associated with disease or harmless (non-pathogenic), referred to as a ‘variance of unknown significance’ or VUS. This is because the change has only been identified in a very small number of people so we cannot determine statistically if it is associated with disease or not.
In summary, 42 of the 100 people with MND in this study showed some form of variants in the 44 known MND-linked genes. 35 of these people had apparently sporadic disease which shows that some familial and sporadic cases can share the same genetic cause of disease. It is important to stress that not all of these changes will cause MND to develop. In fact, many of them may not cause any problems at all.
Blurred lines between familial and sporadic cases
In recent years, thanks to technological advances in reading the genetic code, many risk genes for MND have been found across the world. In some people, changes in particular genes have been identified as an underlying cause of their MND. By reading and comparing the genetic differences in people with MND in families, it has been possible to identify some of the genetic causes of the disease.
However, the situation is still complicated as having a genetic difference doesn’t mean the disease will develop in that person… MND is likely caused by a subtle combination of genetic and environmental ‘risk factors’. We also know that there are several ‘steps’ or ‘events’ that must occur to cause the disease. It has previously been reported that MND is a six-step process, with genes, environment and time (in the form of aging) contributing to disease development, and that genetic components can account for several of these steps in some people. It is almost as though genes build the campfire and environmental risk factors strike the match. For more information see our ‘Steps to understanding MND’ blog post.
The identification of possible genetic causes in sporadic patients is blurring the lines between ‘familial’ and ‘sporadic’ MND. When considering treatment options, the most important factor is the underlying biological cause which if genetic would be the same regardless of whether there is a family history of MND or not. Future studies will continue to see if more verified genetic causes of MND are also found in cases without a family history. Access to AMBRoSIA and NECTAR will enable researchers to delve deeper into the genetic make-up of people with MND, and this recent publication reflects this.
Current state of genetic testing for MND patients in the UK
At the moment in the UK, routine genetic testing of all MND patients is not available, it is only offered to people with a family history of the MND, dementia, or who experience disease onset at a young age. Even then, it is limited to tests for a small number of genes. This is due to several factors:
[tabs] [tab title=”Funding”] The ‘panel’ of 44 genes used in this study is a research tool, but the MND Association has funded this study in anticipation that the experience gained can be used for developing a clinical service in the future. [/tab] [tab title=”Technology”] The technology and techniques required are not routinely available at the moment. [/tab] [tab title=”Genetic counselling”] Behind every sample is a person, family and friends affected by the disease, so it is essential that we are sensitive to the wishes and potential implications of uncovering genetic information about an individual. There is a requirement for genetic counselling prior to, and after, any genetic test as they provide facts and guidance about options. However, studies have shown that the waiting list for genetic counselling can potentially increase diagnostic delays rather than reduce them. [/tab] [tab title=”Trained specialists”] As this research has shown, there are many genetic variants that occur in MND-related genes, but it is not yet known what effect they may have. If genetic testing is to become more routine in the future, it is not just about the test and the counselling, it is also about the highly specialised interpretation of the results so trained specialists are required to understand the difference genetic testing will make to treatment choices. [/tab] [/tabs]The questions of whether genetic testing should be incorporated into the diagnostic process is becoming increasing important as scientists identify more and more genes that are linked to MND. Genetic testing could help improve and speed up diagnosis is used alongside other diagnostic tests. Currently, diagnosis can take on average a year from symptom onset. The earlier a diagnosis is made, the sooner the appropriate care plans and treatments can be put into place.
In addition to this, drug companies are developing approaches to treat MND by specifically targeting associated genes to reduce the damage caused to motor neurons. There are ongoing clinical trials of experimental treatments targeting SOD1, C9orf72 and FUS genes, with other ‘gene therapy’ approaches likely to emerge in the coming years – hence the important of being able to quickly and easily identify the correct participants for these trials.
However, with the advent of targeted gene therapies on the horizon this may need to change, as the evidence presented from the first 100 MND patients in AMBRoSIA shows that some ‘sporadic’ patients could be eligible to take part in trials for the gene therapies that are offered to people with ‘familial’ MND.
To summarise
Quantifying the potential benefits that sequencing of all patients would provide, in terms of benefit to patients in the clinic and potential genetic therapies, has not really been completely measured – until now. This collaborative research effort, in combination with the MND community, is furthering our understanding of the disease.
This work provides rigorous scientific evidence that genetic testing for all MND patients would allow more patients access to more clinical trials. There is an increasing logic to categorise patients based on the underlying cause of their disease because medicines target particular biological pathways and individual genes operate within individual pathways, so it makes sense to treat the individual with medicine based on their particular biology.

“Our study suggests that all patients with MND should, with careful counselling, be offered genetic testing.”
“We hope that by screening all MND patients for gene mutations that are a known factor in MND, we can further our knowledge on subclassification of the disease, but also ensure that patients have access to clinical trials that are relevant for them personally.
“This is increasingly important in light of the new personalised medicine treatments in development for MND that target a specific gene mutation to ensure that patients have access to potential treatments that could be beneficial to them.”
Professor Dame Pamela Shaw, Director of the Sheffield Institute for Translational Neuroscience (SITraN) and the NIHR Sheffield Biomedical Research Centre
What happens next?
Work is continuing to gather data from this valuable resource and the study is being extended to analyse samples from the rest of the AMBRoSIA biobank, helping us understand the biological and genetic signatures of the disease.
“This study was supported by funds raised through the Ice Bucket Challenge with generous additional support from the Linbury Trust, London City Swim Foundation and Credit Suisse UK. The study will be widened to include analysis of additional samples from two other clinics collaborating on this MND Association funded project. This will provide an even clearer picture of the UK MND ‘genetic landscape’.”
Dr Brian Dickie, Director of Research Development at the Motor Neurone Disease Association
In terms of genetic testing, the global MND neurology community is currently wrestling with the pros and cons of routine genetic testing and the challenges that will need to be overcome for this to happen. We are starting to work with UK neurologists to look at current practice across MND clinics, as well as learning from other diseases where genetic risk is involved, to help develop guidance on when genetic testing may or may not be appropriate.
Undoubtedly, a key driver for more genetic testing in the diagnostic process will be the emergence of effective treatments targeting specific genes, as we will hopefully see from the ongoing trials for the SOD1 and C9orf72 forms of MND.
Reference: Shepheard SR, Parker MD, Cooper-Knock J, et al. (2020)
Value of systematic genetic screening of patients with amyotrophic lateral sclerosis. Journal of Neurology, Neurosurgery & Psychiatry. Published: 14 February 2021
Resources:
- Previous blog posts:
- MND Association website:
- News – MND Association-funded study suggests routine genetic testing could have positive impact on care
- Take part in research – AMBRoSIA
- Sheffield press release: New study suggests genetic testing could be appropriate for all motor neuron disease (MND) patients whether or not they have a family history of the disease
As someone with C9orf72 fALS I’ve considered it plain common sense to test all possible MND diagnoses as having a potential genetic mediation. What’s the cost? With more & more genes linked to MND being discovered, isn’t it logical?
Further to my previous comment, since diagnosis nearly a year ago with c9orf72 mediated familial ALS I am surprised that I have not been contacted by anyone in the UK interested in research or clinical trials. My mother, her mother and sister and nephew all with suspected FTD and my son with confirmed c9orf72 mutation. From my statistical analysis of the likely UK population, and the fact that I signed up to MND Smart nearly a year ago and have emailed Sheffield uni researchers, Edinburgh research team, etc I would have thought I would be in some demand. Contrast with ALS TDI in the US who signed me up to their Precision Medicine Program which provides free whole genome analysis, four limb motion trackers,a monthly ALSFSR & vocalisation analysis. Just wondering.